Folate (5-MTHF)
Folate (5-MTHF) is the biologically active form of folic acid. There are two forms of biologically active folate:
- L-5-Methyltetrahydrofolate Calcium, also known by the brand name Metafolin®
In this form, 5-Methyltetrahydrofolate is linked to calcium salt. - • (6S) 5-Methyltetrahydrofolate Glucosamine salt, also known by the brand name Quatrefolic®
In this, the 5-Methyltetrahydrofolate is linked to glucosamine salt.
Please pay attention: possible worsening of symptoms when starting folate
The possible initial exacerbation caused by folate (5-MTHF) can be very serious. Taking this into account is important. A severe initial exacerbation may not only relate to the existing symptoms but can also cause new symptoms.
Common complaints of folate supplementation1 are:
- irritability
- insomnia
- sore muscles and joints
- acne and skin rash
- severe anxiety
- palpitations
- nausea
- headache and migraine
Slowly increase dose
When taking folate (5-MTHF) it is important to start slowly with 100mcg once a day. We strongly recommend you do this in consultation with a therapist. Overview therapists
For folate, currently the same upper limit is used as for folic acid:
| Age | Upper limit (in mcg a day) |
|---|---|
| 0-5 months | 85 |
| 6-11 months | 130 |
| 1-3 years | 200 |
| 4-8 years | 350 |
| 9-13 years | 600 |
| 14-18 years | 900 |
| 19 to >70 years | 1000 |
| Pregnant | 1000 |
| Breastfeeding | 1000 |
The optimal daily dose differs per person; 100mcg can make the difference between a positive and a negative reaction to folate. This means you may respond well to 400mcg a day but get negative symptoms when taking 500mcg a day.
Therefore, it is important to set an optimal daily value. Start with taking 100mcg a day and keep a close eye on your complaints. If your symptoms get worse, you can stop taking folate for a week before continuing it again. If the symptoms are experienced as severe, contact your physician immediately.
When your symptoms do not progress after taking folate for a week, you may increase your daily dose to 200mcg. Then again, when your symptoms do not progress, you can increase your dose to 300mcg a day. This weekly increase, which can only be made when there are no complaints, can be proceeded until the optimum daily dose is found. You should keep the maximum upper limit in mind. If your dose is too high, symptoms will reappear and the lower dose may be obtained as an optimal daily dose. If necessary you may stop for a short period of time before reintroducing your optimal dosage. The body never rests, certainly not during treatment. As a result of this, the optimal daily dose can vary over time.
Genetic mutations folic acid conversion
Research has shown that the conversion of folic acid and dietary folates into active folate isn’t optimal in about half of the European population.4
This has to do with a genetic mutation called C677T in the MTHFR gene. The MTHFR gene is required to convert folic acid into active folate. The genetic mutation C677T leads to a 30 to 45% reduction of the activity of the MTHFR gene. This means that it will take longer for the body to convert folic acid and dietary folates into the biologically active form of folate. In the Netherlands, about 40% of the population suffer from the gene mutation C677T. 4,5,6,7,9,10 This does not necessarily have negative effects, but it can be an explanation for existing complains.
Another common genetic mutation in the MTHFR-gene is: A1298C. This gene mutation leads to a 10 to 32% activity reduction of the MTHFR-gene.4
If you suffer from both gene mutations, the activity of the MTHFR-gene is reduced by 60 to 70%.11 Between 5 and 10% of the population seems to suffer from both gene mutations. A common occurrence of both gene mutations is a high homocysteine value.4
High homocysteine value
A high level of homocysteine damages the inside of blood vessels, which leads to a considerably higher risk of:12,13
- coronary heart disease
- heart attacks
- brain haemorrhages
- strokes
- blood clots (lung embolism, deep vein thrombosis)
- stenosis of the carotid- and renal artery
- aneurysm (dilatation of an artery)
MTHFR-gene
Due to the strongly reduced function of the MTHFR-gene methylation is less effective, which leads to a high level of homocysteine. Methylation regulates the production of:- DNA
- RNA
- Basis proteins
- Lipids (fats used for, for example, cell production)
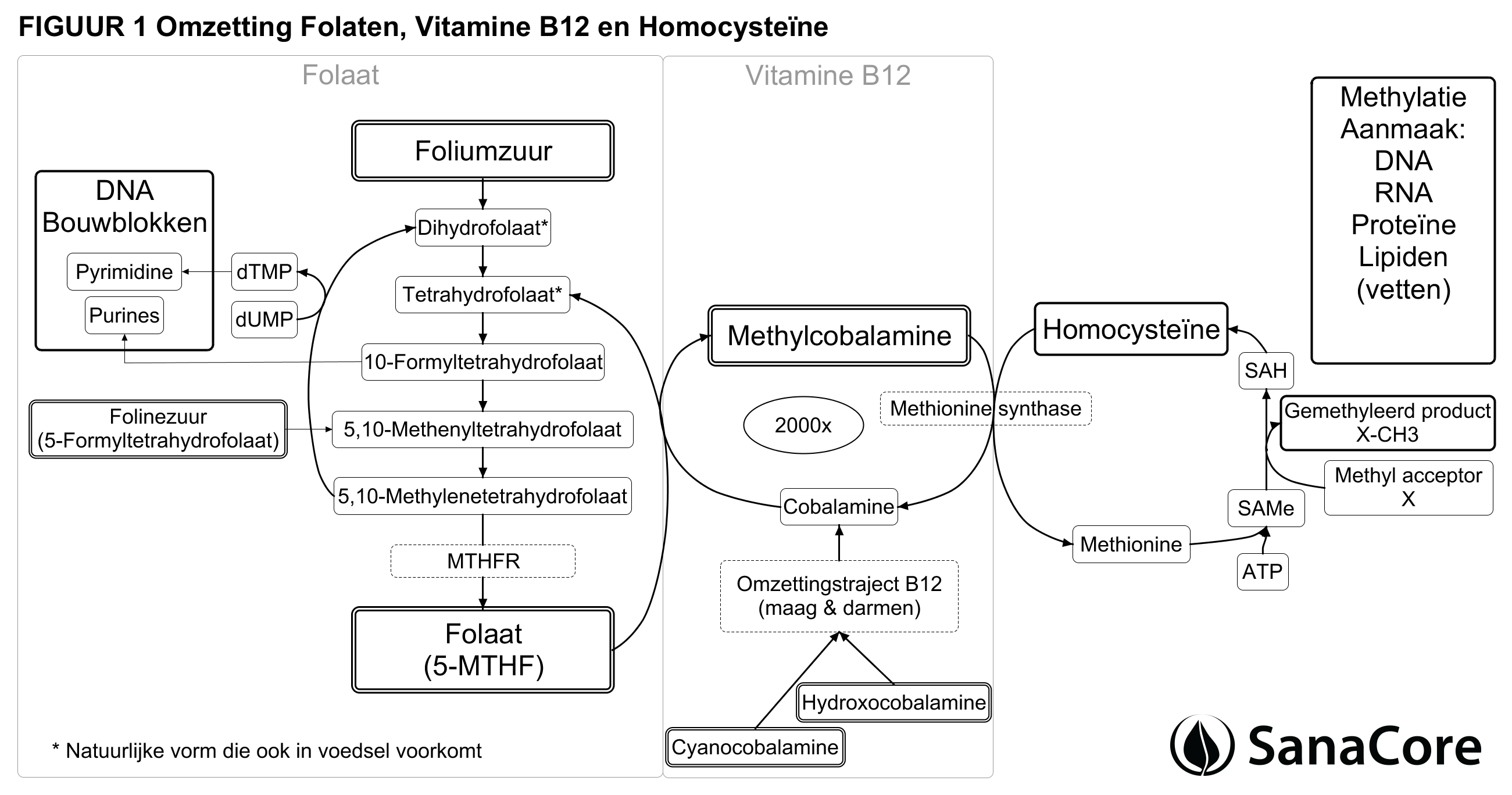
FIGURE 1 Conversion of folates, vitamin B12 and homocysteine 17, 18, 19, 20, 21
{kind=link}
Vitamin B12 and folate or folic acid
As can be seen in FIGURE 1, vitamin B12 and folate (5-MTHF) use each other to convert homocysteine. Vitamin B12 (cobalamin) can be reused up to 2000 times because of folate. Folate releases a methyl group in order for vitamin B12 (cobalamin) to be converted into methylcobalamin B12. 17Supplementing vitamin B12 without folate or folic acid will lead to decreased levels of folate. Conversely, when solely taking folate of folic acid the B12 level will decrease. An insufficient amount of folate or free cobalamin will stop the whole process, leading to a rise of homocysteine.17
Methylcobalamin B12 does not have to be converted by the body, because it is a biologically active form, therefore it is an ensured supplementation for vitamin B12. This is also true for folate (5-MTHF), which is biologically active and therefore an ensured supplement17
The cooperation between folate and vitamin B12 enables folate (5-MTHF) to be converted into tetrahydrofolate. When tetrahydrofolate is being converted back into folate (5-MTHF) essential elements for DNA are made: Purine & Pyrimidine.18
Dietary folate
“Folate” means “leaf ” in Latin. Folate is mainly present in: dark-leaved green vegetables, citrus fruits, dried beans, peas, liver, poultry, pork, shellfish, grain bran and other whole-grain products.19 When following a varied diet, you usually have a sufficient intake of folate.20
As can be seen in FIGURE 1, dihydrofolate and tetrahydrofolate (dietary folates) are lower on the list than folic acid, which indicates a higher bioavailability.
However, dietary folates have two major points of attention:
- Folate is very sensitive to temperature, it is estimated that 50 to 95% of the folate present in food is lost during cooking. When processing cereals (refining), all of the present folate is lost.22,23
- Dietary folate passes through the gastrointestinal tract, where a lot is lost as well. Comparing to folic acid, 30 to 80 percent of the ingested folate is absorbed.26 The acidity of the intestine also influences this. If it is too low, less folate is absorbed.25
To lower homocysteine levels, folic acid is much more effective than dietary folate. Where 200mcg folic acid per day can bring the value of Homocysteine down with more than 1.5th point after one month, 200mcg of dietary folate only decreases this value with about half a point. 26
Folic acid
Folic acid is converted by the liver into the natural forms of folate: Dihydrofolate and eventually tetrahydrofolate.27
Part of the folic acid in the liver is excreted through the bile, but most of it is then reabsorbed through the enterohepatic circulation.25, 28
Folic acid and interactions26:
- Vitamin C stimulates the absorption of folic acid
- Alcohol disrupts the reabsorption of folic acid from the intestine
- Laughing gas disrupts the absorption of folic acid
Folinic acid
Folinic acid is a more active form of folic acid, but still depends on the MTHFR-gene for its conversion into folate (5-MTHF). 20
UMFA’s
UMFA stands for unmetabolized folic acid. These can occur in different forms. Generally, they exist in -folic acid supplement- form and 5, 10-Methylenetetrahydrofolate-form.
5, 10-Methylenetetrahydrofolate is converted into the biologically active folate (5-MTHF) by the MTHFR-gene. A reduced function of the MTHFR-gene may influence the level of 5, 10-Methylenetetrahydrofolate UMFA’s.
UMFA’seem to be correlated with folic acid intake, but this correlation is not entirely clear yet, because folic acid intake alone cannot explain all differences in UMFA levels 31,32,33 there might be a relation with vitamin B12.34
Several studies indicate that a high level of UMFAs, due to high folic acid intake, should be a point of attention because of the possible adverse effects.35,36,37 However, there is no conclusive evidence for this yet.
A low level of UMFA’s does not seem to be harmful.29,3 It might even have benefits.36 Folate (5-MTHF) does not appear to influence the level of UMFA’s or any of the possible adverse effects.36
One study indicates that in mice a large amount of folic acid causes a reduced MTHFR function which results in a low folate (5-MTHF) level. 37 37 But this study does not provide conclusive evidence and it calls for additional research.
Folate (5-MTHF)
It seems as if folate (5-MTHF) can improve low folate status as effectively as folic acid can.30
As far as we know, there are no harmful side effects of folate (5-MTHF). Moreover, taking this supplement does not lead to less UMFA’s.2Folate (5-MTHF) supplements have a positive effect on the folate status of the body and decrease the level of homocysteine.38
Tests
It is possible to be tested for the genetic disorders C677T and A1298C. You can request these tests through 23andme.com, costs: £145.
The homocysteine test can be requested at your general practitioner or via ProHealth.
Conclusion
There are two options for supplementing your folate levels: active folate (5-MTHF) and folic acid. It is important to take either of these in combination with methylcobalamin B12.
Choosing for active folate (5-MTHF)? This form is definitely well absorbed in the body. Slowly increase the daily dose and keep a close eye on the possible symptoms that may be related to it. We strongly recommend only taking this supplement after consultation of a therapist/health professional.
Choosing for folic acid? Folic acid is included in all our packages. We have seen good results with folic acid for years now. When starting to take folic acid there is no possible worsening of symptoms. If, however, the desired vitamin B12 reaction does not occur, it is possible your body does not convert folic acid properly. In this case, switching to folate (5-MTHF) might be the answer. Naturally, this switch should be in consultation with a therapist/health professional.
It might be interesting to get a homocysteine test done before and after taking supplements for one month, to see if the homocysteine value is decreasing. If this is not the case, this could be an important sign that you’re your body is ineffectively converting folic acid into folate (5-MTHF).
Recommended literature
Could it be B12? Sally M. Pacholok
Chapter 5: Stroke, heart disease, and other vascular problems: the B12-homocysteine connection
Chapter 7: Vitamin B12 and cancer, impaired immune function, and autoimmune disease
List of therapists
- Contact
- Terms and Conditions
- Sitemap
- Privacy policy
- Disclaimer
- © VitaminB12first 2025